Happy Winter Solstice! Wait, can I say that? Do we get to enjoy it?
Honestly, I can't. I am having a hard time enjoying anything anymore, because I'm watching everything around us quickly crumble and decay. This year brought a lot of destruction that may not have been able to be prevented (see: massive hurricanes, earthquakes, wild fires, volcano eruptions), but could have been tempered with the simple belief in climate change. The scientific community's throats are sore from yelling "PLEASE BELIEVE US", and our eyes our tired from writing grant after grant after grant begging for adequate funding to find ways to minimize the destruction and better our outcomes.
In this season of light, everything is dark. There is no hope left for the new year, because we are being told to shut our mouths and follow the rules set by people who don't have the proper training, expertise, or even a hint of interest in anything but themselves.
Let's talk about the utter travesties for the sake of watching the avalanche unfold one more time:
From the day of his inauguration, He Who Shall Not Be Named began stripping credibility from the scientific community within the US. The climate change section of the white house website was removed entirely, not to show change, but to show complete erasure of progress. The "leaders" of this country fail to see that the health and wellness of your environment is the new space race, the new cold war. Everyone is racing to undo the damage of decades of ignorance, yet here we are, stuck at the starting line because we can't even agree on a common goal.
Access to reproductive health care was a constant battle this year, as many of the female-forward initiatives tied into Obamacare would have been threatened with the repeal. On top of that, immigration and reproductive rights overlapped with cases of state and federal attempts to deny patients access to their choice of care. Brigitte Amiri of the ACLU commented “With this case we have seen the astounding lengths this
administration will go to block women from abortion care. We will not
stop fighting until we have justice for every woman like Jane.” Unfortunately, history always tells us that this issue in particular will be a never-ending battle, especially with disrespectful trash leading the way.
Planned Parenthood representation at the Women's March 2017, via HerCampus
US citizens that inhabit Puerto Rico were simply told to help themselves after being hit by two unbelievably massive hurricanes, one right after the other. This response, after the outpouring of love for Houston, which was also hit extremely hard, was the white house's way of saying "you're brown, so you don't count". Let's do ourselves a favor and NEVER LET THAT SENTIMENT BE SAID OR IMPLIED EVER AGAIN.
Science funding was a ridiculous mess, with He Who Shall Not Be Named and Congress not agreeing, and the outcome being...kind of all over the place. The biggest laugh comes from He Who Shall Not Be Named trying to cut NASA's funding, and then stating later that immediate future initiatives will be to go back to the moon, instead of previous calls for Mars in 2020.
An idiot looks directly at the solar eclipse that happened earlier this year.
Also in November, we are allowed to give thanks to those who stole the land that this country was built on by celebrating the proposal of national monument land reduction -- the largest in US history. Nothing is sacred, everything will be doused in oil and profits. The future of our national parks includes drilling and mining.
Kenya Wildlife Services ranger guards illegal ivory, via LA Times
The latest GOP tax cuts, passed in December, initially threatened to tax graduate student tuition fees that are waived as a part of their programs agreements, but didn't end up in the final, passed version. That's not to say most students seeking higher education wont have a harder time accessing and paying for it.
As far as public health is concerned, how can we lead preventative efforts if we may not be able to say certain words? A flood of news stories claimed that the CDC had a list of banned words that they are not allowed to use, which includes "fetus", "vulnerable", "diversity", "entitlement", "transgender", "evidence-based", and "science-based". That claim has since been denied, but we'll see how things change.
I'm clearly skipping over a lot of stuff just to highlight the science-heavy hits of this year. We can also tie a nice bow on this list with all the outbreaks that occurred this year. You'll notice many of the diseases on that list are vector-borne diseases, the spread of which has been proven repeatedly to be influenced by changes in climate.
With each passing day, the situation worsens. I can link Betsy DeVos to the destruction of scientific and technological advancements in the future because STEM education will wither under her care. Challenges with our changing climate will continue to worsen, because we are not training the minds of the future to think creatively about how to tackle such problems -- or even that such problems exist, as many science textbooks don't include sections realistically representing climate change.
Everything feels like its crumbling right now, and I already feel like I know what's coming in the new year.
Happy holidays, whatever you believe in or celebrate or do this time of year.
Find some hope for science somewhere, please.
On Monday, I attended a symposium, titled "One Health: Interface of Human Health/Animal Diseases", at the American Society for Tropical Medicine and Hygiene (ASTMH) annual meeting (aka #TropMed17). This was one of many sessions I attended, but one of the few that really stood out to me.
I love the concept of One Health, which emphasizes the interwoven nature of the environment, animals, and humans, where a change to one aspect of the world will affect the other surrounding environments and populations. This is a vital concept when it comes to global health, as we often focus on human disparities without working to improve the person's environment for sustainable health and change. As you can imagine, One Health is a critical component when describing the lifecycles of zoonotic diseases, which infect both animals and humans. I wrote a magazine article for The Biochemist about the impacts of One Health on disease emergence. You can find that here (e-zine) or here (PDF), for free.
Within the One Health symposium, each speaker outlined an important animal exposure for each infection, whether parasitic, viral, or bacterial. For example, the first speaker discussed an outbreak of hantavirus in Peru during the creation of a new interoceanic highway that runs across Peru and Brazil. Deforestation and construction created a new opportunity for exposure to hantavirus for construction workers and residents in the area. Here's some more info on that, if you are interested.
Another speaker spoke about emerging pathogens in Myanmar due to exposure to bats through the use of caves for economic (mostly the creation of tours for tourists) or religions purposes (think shrines in caves). Myanmar apparently has 22% of world's species of bats, meaning it has a diverse population of bats, and they are everywhere.
The two talks that I really enjoyed covered parasitic infections that are a global issue affecting primarily low income populations, even those in the United States.
Angiostrongylus cantonensis, or "rat lungworm",is a parasitic nematode that is found throughout Southeast Asia and the Pacific basin. Rat lungworm causes eosinophilic meningitis in humans. Humans are exposed to A. cantonensis through ingestion of infested foods, like undercooked or seafood, fish, frogs, vegetables, or snails.
Apple snails act as a reservoir for A. cantonensis throughout Southeast Asia. Upon investigation, the larval stage of the nematode can be found invading the lungs of the snail. Adult A. cantonensis live in the pulmonary arteries of rats, and larvae migrate to the pharynx, where they are swallowed by the rat and dispelled in the rat's feces. The larvae are then ingested by the apple snail, or other specific mollusk species.
The apple snail can be purchased to eat from stands along the road in Laos, Cambodia, and Thailand, or the larvae can infest other aquatic animals. Once ingested by a human, the nematode travels to the brain through the blood stream, and then dies shortly after. The presence of a foreign body in the central nervous system causes a flood of white blood cells, specifically eosinophils, which triggers inflammation of the meninges. While this can clear on its own, some people have been seen with significant neurological dysfunction, some of which are lifelong, or death. This parasite is most commonly associated with Southeast Asia, in the past few years, has popped up in Hawaii.
Another speaker detailed a project focusing on parasitic load in public parks throughout New York. Toxocara spp. can infect dogs (Toxocara canis) and cats (Toxocara cati), and can also infect humans if the eggs are ingested. I think a lot of people in the US believe that parasites are a problem in other countries, but there are many types of parasites that can infect (and infest) people in urban and rural areas of the US.
Toxocara roundworm image from the CDC
Toxocaraisis, or an infection caused by Toxocara spp., is a roundworm infection that causes symptoms depending on where the larvae migrate in the body. Visceral toxocariasis occurs when the larvae migrate to various organs, most commonly the liver or central nervous system, causing fever, fatigue, coughing or wheezing, or abdominal pain. When in the central nervous system, psychological symptoms and neurological dysfunction can occur. Ocular toxocariasis occurs when the larvae migrate to the eye, causing symptoms relating to the eye, such as vision loss, inflammation of the ocular tissues, or damage to the retina that can cause permanent blindness. The CDC estimates that up to 70 people are blinded each year from Toxocariasis. Many people clear a Toxocara infection without experiencing any symptoms, and have a strong immune response.
This particular project tested soil and sand samples from parks because children are frequently exposed by ingesting soil and sand from parks, and from putting contaminated hands in their mouths. Infection during childhood can affect childhood development, and most people are never diagnosed if they don't present with severe symptoms. Many psychological symptoms aren't linked to parasitic infection, so they aren't treated appropriately!
Some random kid from the internet eating dirt.
More importantly, the presenter emphasized how this is an infection that is more common in low income communities. For example, out of all the areas tested throughout New York, parks in the Bronx had significantly high contamination levels (something like 67% of parks tested in the Bronx had positive samples!). The CDC estimates that ~14% of people in the US have antibodies against Toxocara spp., suggesting that tens of millions of Americans have been exposed to these parasites at one or more points in their lives.
The presenter's data, combined with the CDC's estimates of exposure in the US, suggests that a majority of those exposed to Toxocara are from disadvantaged communities, where public health initiatives fall short. This means that health services are not doing their jobs to protect all people within a community. We can't just protect select groups. All people have a right to be informed of what they may be exposed to in their local environment, and what local organizations (whether nonprofits, government organizations, or research initiatives) are doing to minimize risk!
If you are interested in this specific project, here is an older youtube video of the speaker describing her research:
Its important to remember that the concept of global health affects people around the globe, especially children, no matter where they live or how developed their environment is. Public health interventions have helped reduce the number of diseases that many people in developing countries would be exposed to, but no one lives in a sterile environment!
It’s starting to get really hot as summer sets in for many regions of the world. Even in the last weekend, we had temperatures of 100F throughout the Bay Area (where’s my “June Gloom”?). Over the last decade, we have seen record-breaking temperatures and drastic changes in seasonal climate, in which only some people believe are actually real and worthy of concern. When we think of summer, many people try to make the most of the longer hours of daylight and more palatable temperatures by spending more time outdoors. This simple act of migrating towards wilderness, combined with shorts and tank tops, makes for a memorable “meet-cute” scenario, only instead of casually encountering the love of your life, you’re mingling with vectors that harbor disease.
My husband often calls me a buzzkill because I can’t help but interject when friends, relatives, or acquaintances tell me that they are planning a summer trip to a location that I know is endemic for one, two, or many vector-borne diseases. “I hope you are bringing some DEET,” I say, explaining that all of the information you need is conveniently located on the travel.state.gov and CDC websites. People often get pissed off when I suggest they take precaution instead of flaunting the new swim suit they’ve purchased just for this trip. Whether they take my advice or not is completely their choice, but I can’t help but feel like I’d be partially liable if I didn’t at least warn them.
Many people are still afraid of traveling to tropical islands and throughout South America, as Zika is still in recent memory, and many parts of Europe, for fear of being attacked by a terrorist. Instead, people are opting to explore the natural wonders in their own “back yard”, stating that it’s not only “cheaper, safer, and less of a hassle”, but also that they are afraid He Who Shall Not Be Named might start selling off our National parks for industrial use and that they’ll miss the Instagram photo-op forever if they don’t go now.
Are we really safer in the United States? Sure, there are many reasons to believe that, from an infectious disease standpoint, we are. We haven’t had autochthonous malaria here since the days of our founders, and most people have access to and choose to get vaccinated.
But people die or suffer from chronic conditions as a result of infectious diseases here all the time, many of which can be prevented with basic action.
I write about tick-borne diseases almost every summer, and for good reason. Tick-borne diseases are spread by ticks, and come in the variety of flavors. Many are treatable if caught before chronic illness sets in, as with Lyme disease, but there are still some that cannot be treated. In all cases, the tantamount risk lies with getting bitten by a tick. Without the tick, you can’t get an infection. It’s as simple as that.
Beautiful image of a blacklegged tick from coppelabs.com
But we all do things that we shouldn’t. I’m guilty of it too! I run my local trails in a t0shirt or tank top, risking tick bites every time I do it. Why do we refuse to let these vectors take control of our lives? Confidence, maybe? Blissful ignorance associated with a “that won’t happen to me” attitude? I’m not sure.
With that little diatribe, let’s talk about Powassan virus, or “POW” for short. POW is an RNA virus from the genus flaviviridae, meaning it is related to many well-known mosquito-borne viruses like dengue virus, West Nile virus, and yellow fever virus. POW is definitely a lesser-known tick-borne disease, because I think most people only have space for Lyme disease in their cerebral storage. There have only been 75 confirmed cases of POW infection in the US in the last decade, so it’s not as sexy to the news as larger outbreaks. Yet, it’s one to note, because there are no treatments available, aside from symptomatic treatment. According to the CDC, POW neuroinvasive disease cases have been reported in Maine, Massachusettes, Minnesota, New Hampsire, New Jersey, New York, Pennsylvania, Virginia, and Wisconsin between 2006 and 2015.’’
That’s right, it’s a neuroinvansive disease, which means after being bitten by an infected tick, the virus can infect the central nervous system, causing encephalitis and meningitis. Upwards of 10% of cases are fatal, and the CDC reports that approximately half of those infected suffer from permanent neurological symptoms.
Image from webmd.com
Not only does the warmer weather drive humans outside, it also expands the territories where many vectors, like mosquitoes and ticks, can survive and thrive. As temperatures increase and stay warmer longer, tick populations have expanded, increasing the likelihood of being bitten. Many predict that there will be a dramatic increase in the number of POW infections this year, as weather continues to warm.
There is no treatment available for POW infection, aside from symptomatic treatment. Since POW is a virus, the antibiotics used for Lyme disease won’t work on a POW infection. Yet, most people who are infected are asymptomatic, and won’t experience any of the symptoms of POW disease. POW isn’t transmitted from person to person, so there’s risk of unknowingly infecting others if you are infected.
If you’re planning a camping or hiking trip, or you’re an avid trail runner like me (and by avid, I mean, I’m amateur at best), I suggest reading over these tips on preventing tick bites, and remember that POW cases have only been detected in the northeastern states, and around the Great Lakes.
If you do find a tick on you, here’s a video that shows how to remove a blacklegged tick:
I know I'm a little late to the Valentine's-themed blog update game this year (and, like, every year? Let's be honest), but I was busy celebrating a general feeling of love in my life by grading midterm exams all night long. But, in honor of St. Hallmark (har har), I'd love to tell you about an unforgettable kiss.
South America is famous for romance and religion; two concepts that seem to overlap regularly throughout history. Given the tropical climate that engulfs Central America and most of South America, and the common built environments (housing structures, etc.) in rural areas, South and Central America are also endemic for a number of neglected tropical diseases. For example: despite the fact that a yellow fever vaccine exists, there is a huge yellow fever outbreak happening in Brazil right now. This just shows that with the right environment, if preventative measures (like vaccines) aren't required, then the disease will prevail.
Aside from our well-known and beloved mosquito vector, Central and South America are also home to an incalculable abundance of other insects that have the ability to spread many different diseases. One of my favorites (so to speak), is the triatomine bug, AKA the "kissing bug" or the "assassin bug".
Triatomine bug on a knuckle. Image borrowed from The Tico Times
These relatively large insects are bloodsuckers, meaning they take a blood meal from mammals. Due to their need for blood, land clearing, and human encroachment into heavily forested areas, many species of triatomine have adapted to living in and around housing structures. This environmental cross-over helped our friend, the triatomine bug, to start transmitting a number of diseases. The most common disease they spread is the protozoan parasite Trypanosome cruzi, which causes Chagas disease.
Trypanosome cruzi next to a red blood cell. Image (c) to Pearson Education.
Triatomine bugs, known for the unforgettable kiss I mentioned earlier, are nocturnal and attracted to carbon dioxide, which we emit constantly as we exhale. Humans exhale the highest concentration of carbon dioxide in one location while they are sleeping, because most people don't move around as much while they are out cold.
After biting an infected animal or human, the bug now contains the parasite and is able to transmit it to another being. The infected bug bites and draws blood for a blood meal while defecating on the surface of the skin. The bite is usually painless and doesn't wake the latest victim.
By including the act of defecating during feeding, the triatomine bug deposits T. cruzi onto the skin. A combination of the irritation of the bite, and a mild allergic response to the feces, causes the skin to feel itchy. Scratching the itch helps move the feces and parasites into the bite wound, and infection ensues. After scratching, the parasite can also make their way into the body via mucosal tissues in the eyes, nose, and mouth, reaching the bloodstream through penetration of the delicate tissues. The parasite needs the triatomine bug to break the skin, since it is too thick for the parasite to penetrate on its own.
This complete life cycle diagram is courtesy of the CDC.
Fever and swelling of the lymph nodes kick off the presentation of symptoms. A sore may develop at the site of the infection, and if the person was bitten on the face, a presentation called Romaña's sign causes distinct swelling around the eye. Romaña's sign occurs in approximately 50% of infected individuals, and is often considered one of the tell-tale signs of infection.
Romaña's sign in the left eye, image from the WHO and the CDC
If not treated during the acute phase of infection, after initial symptoms subside, the chronic phase of Chagas disease sets in. Chronic Chagas disease can cause major complications to organs and entire organ systems, such as irreversible damage to the heart, intestines, and liver. Its estimated that over 25% of infected individuals develop potentially fatal damage to the heart.
Treatment for Chagas disease is usually a combination of benznidazole and nifurtimox, anti-parasitic medications that attack T. cruzi. This treatment must be given during the acute phase, when the parasite can be found in the circulatory system. In endemic regions, treatment is typically available. Yet, in the US, you must have a confirmed diagnosis of Chagas disease in order to obtain the treatment from the CDC, because it is otherwise not available. Diagnosis is performed by a blood smear viewed with a microscope to identify the parasite in the blood. Other tests, such as PCR, can be performed, but the blood smear is the gold standard in identification and diagnosis.
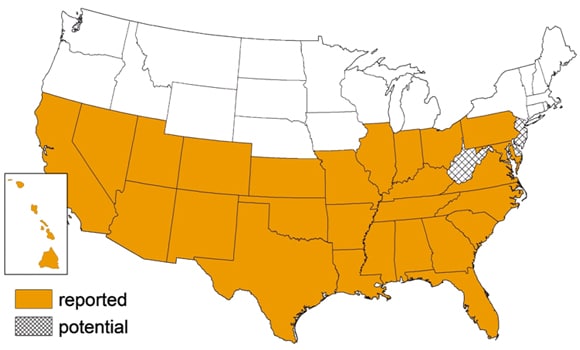
Triatomine bug populations reported in the US, via the CDC
The vector, triatomine bugs, are found throughout a large part of the southern US. A small number of locally-acquired cases have been reported, but not enough to cause huge alarm. Also, there are a number of ways this parasite can fail to infect you.Without the presence of the vector, the parasite cannot infect you. The parasite cannot penetrate the skin on its own, so unless a triatomine bug successfully bites you, or you have an open wound that is exposed to the feces of triatomine bugs, you are not at risk. Additionally, triatomine bugs don't always defecate when they feed.
The best way to limit exposure to Chagas disease is by reducing your exposure to the triatomine bugs, since there is no available vaccine, and treatment can be difficult to obtain in the US. Monitoring your house for triatomine bugs, cleaning away debris to reduce environments for their ideal hiding places, and if you are truly worried, regular insecticide spraying can all reduce your risk of exposure. While most insecticides have not been approved for use in the US against triatomine bugs, long lasting insecticides have been shown to kill them.
I haven't posted anything in a while, simply because the last few months have been occupied with self-reflection and constructing a plan of action for 2017. After the US Presidential election results were released, it seemed like a waste of time and energy to write about some disease that most people in the US will never even learn about, let alone be exposed to.
I was caught in an ambiguous fog of wondering whether the work that I do (my research, not necessarily this blog) is truly worth it, or if I'm just contributing to the unsustainable aspects of "global health". It can be frustrating when your subjects are on another continent, in another time zone, and will never interact with you face-to-face. Its also frustrating when you realize that you are just another white lady that claims a passion for global health/"wanting to make a difference". What does that mean, really? And frankly, what does that mean now that our government is lead by someone who believes in business over, well, everything else?
Community health workers in Madagascar (photo from K4Health)
How do you cope with being a person of the scientific community who wants to help initiate positive change, such as expanding the development and access to treatment and vaccinations for neglected diseases, improving access to clean water and sanitation technologies, or expanding educational and economic opportunities for young women in developing countries (just to name a few popular and reoccurring themes in global health), but also realizing that you may be forcing a very biased view on communities that are rarely empowered, but instead labeled has victims? (example: Many journalists claimed the cause for the last, explosive ebola outbreak was initially due to "ignorance" of the affected communities). Similarly, how do you prioritize issues abroad when there is so much happening in your local communities?
I recently finished reading Sometimes Brilliant, by Dr. Larry Brilliant, which details his journey through being a hippy MD with a passion for social justice and civil rights, and how he managed to find a spiritual connection to India while working to eradicate smallpox. On a number of occasions in this story, Dr. Brilliant (lovingly nicknamed "Dr. America" by his guru) questions his actions and whether his efforts are actually helping people in the long term, or if he's contributing to immediate yet unsustainable aid. This obviously spoke to me on a number of levels, but didn't help guide me to a solution (the answer isn't always broad and right in front of you, I guess).
Dr. Larry Brilliant (center) in India in the 1970s, working to educate communities and eradicate smallpox.
The beginning of the year coincides with my birthday, and instead of setting resolutions, I try to revisit the actions I've taken in the last year, and reflect on whether I'm having enough of an impact, giving enough of myself (energy, time, money, values, etc.) to others. This year, I wasn't feeling great about it, because I feel like there isn't enough time in one day, or even one year, to give enough of oneself to a cause (or causes) that will result in a true impact, a change, an improvement.
This dilemma is amplified by the fact that I spend a majority of my time and effort working in a lab at one of the most well known, private universities in the world, wherein I primarily interact with other white people, and everything sparkles with privilege and ongoing gifts from wealthy donors. Despite being in such an environment where low-income students get to attend for free, or where new and extensively valuable discoveries are made regularly, I'm not working in the hospital directly, where I could leave my workday feeling like I had a direct impact on someone's quality of life, or interacting with the students, who will go on to spread their expert educational experiences to many parts of the world with their future careers. When you work in such an environment, it is not clear who is "on your side" politically, or who is there to make a difference versus for the prestige of working with such a well known university. Its easy to feel isolated in a well-off environment when you are aware of inequalities.
Earlier this week, I attended a Global Health Symposium. It was a great event last year, but I wasn't expecting anyone to speak about the real issue at hand: How can we navigate global health issues with the new switch in government? It is typically not talked about, because you never know who voted for which party, or who actually believes the wall should be built. But without discussing such issues, it can make you feel like you are a part of the problem just by going to work.
The opening keynote address was given by Diana Chapman Walsh. Dr. Walsh was president of Wellesley College until 2007, and currently serves on the board of the Broad Institute of MIT and Harvard. She is also on the board of directors for the Mind and Life Institute, where she gets to work with the Dalai Lama. At first look, admittedly, I stereotyped and judged her. I thought, "she appears to be another 'rich white lady' who will talk about working together and doing good things for people of the world, but her talk will be empty and uninspired", because that's how jaded I've been feeling about everything lately. I was clearly desperate for inspiration and guidance.
She proceeded to talk about the urgency of collaboration and navigating our resources while we still have access to them. Stating "they told me I could be political", she spoke outwardly about how white supremacy has put us in our current position, and how it is a danger for the future of global health. Frankly, white supremacists do not value the health and wellness of other, non-white/non-(North) Americans. How does that view impact the health of our nation, and the health of people around the world? Negatively. This new administration is not going to value the federal organizations that perform research and provide aid that benefits people worldwide, as 'they should be able to take care of themselves'. Statements like these do not acknowledge that there is a monopoly on resources that are a fundamental human right. Instead, these resources are traded strategically, doled out as bribes for economic advantage (example: mining natural resources in Africa, trading access to such resources strategically for money and power). Don't even get me started on the white supremacist view of developing countries through the narrow lens of tourism and hospitality industries (Dr. Walsh didn't touch on this, but I bet she has thoughts about it).
Dr. Walsh spoke of climate change as a vital component of global health, which is not a view you hear regularly. You hear of polar bears losing their habitat, and small island villages being swallowed by rising sea levels, but with the polarized nature of climate change, no one likes to talk about the increased spread of disease, how it is affecting animal populations, or how it is going to get extremely difficult for some regions to access basic resources, like clean water and food. Why would you allocate funds for research and innovation to combat these problems if you don't believe in climate change? Also, why would you believe in climate change when you cant see past your own bubble?
A bad photo of an inspiring talk.
What especially surprised me was how Dr. Walsh openly expressed her support for Black Lives Matter. I have never heard anyone at our university (outside of my immediate lab group) express such views openly. It hit me like a punch in the face, because I thought she was going to be someone who wouldn't take a stand, and who would most likely be an expert at straddling the fence. But, no, I was wrong! What a refreshing surprise! She used her position of power to say that we need to consider our local communities as a part of our global health initiatives. What that showed me is that we can be an example, and we shouldn't keep quiet. Also, maybe if we start listening more, we can learn how to get things done? Here's an article that details "8 Black Panther Party programs that were more empowering than federal government programs", just as one example.
A few people referenced the latest Oxfam report on inequality that states "62 people own the same as half of the world", and 53 of them are men (surprised?). Only until the end of the day was the concept of engaging these powerful few for philanthropic endeavors. I mean, look at what a tremendous impact Bill and Melinda Gates have had on research, innovation, and impacting global health. It just has to be seen as a priority.
So where do we go from here? Which causes are you passionate about? How do we harness these ideas for fuel for our activist fire? I hesitated to use the word "activist", but then realized that standing up for global health means being an activist for social justice, no matter where your efforts are targeted.
In a specifically memorable moment of Dr. Brilliant's book, he tells a story about being caught in the middle of a dilemma: to play the game of corruption that may lead to long-term support for their smallpox eradication mission, or to stand up for noble action and do what is immediately right for the cause. He sought guidance from another spiritual leader and was told to consider the question "how are my actions affecting the children who are sick and dying from smallpox?" with every move. Truly how do you navigate these situations when there is a business side to global health? We cannot always only lead with our hearts, because funding will run out in a flash.
I'll still cover infectious diseases, but the tone of my blog may change. There will be more calls to action, for sure. Global health is not only up to the righteously motivated or the extensively educated, especially when we consider global health as all encompassing.
Thanks for the much needed inspiration, Diana Chapman Walsh and Larry Brilliant. I'll see you on the front lines.
This one's for you, Trump:
Note: I've received a number of requests to do a series of posts about vaccinations: how they are developed and manufactured, how they work, etc., so I will be dedicating my next few updates to that subject.