In 1944, a tick-borne virus characterized in Crimea was name "Crimean hemorrhagic fever virus", yet 25 years later, the vector was identified in the Congo. Hence, Crimean Congo Hemorrhagic Fever, or CCHF for short, was born (in the "I've given this naturally existing thing a name so it shall be seen as new" sense). As all vector-borne diseases are limited by the regional distribution of their vectors, it is no surprise that news outlets are currently describing CCHF as a "new" viral disease. Spread primarily by the
Hyalomma species of tick, CCHF has been historically limited in spread, with cases primarily showing up in certain regions of Africa, the Middle East, Eastern Europe, and some parts of China.
Let's look at some older maps that contrasts the distribution of the
Hyalomma species and historical cases of CCHF:
There are a number of factors that have contributed to the spread of CCHF virus. CCHF virus is a zoonotic virus, meaning animals, such as livestock and domesticated animals, may also be infected. Many species of birds appear to be resistant to CCHF virus, with the exception of ostriches. Outbreaks have been linked to ostrich abattoirs (or slaughterhouses) in South Africa, but the animals do not present with disease symptoms or consequences. Primarily cattle, goats, sheep, camels, and hares or rabbits are susceptible, and act as the amplifying host. Humans can become infected as a result of contact with an infected animal tissue or blood, so it is easy to see why herders and abattoir workers are at high risk for exposure. Human-to-human transmission is possible through contact with infected bodily fluids, which puts health workers at risk as well. Cases have been traced back to exposure through contaminated medical equipment, although that is fairly rare.
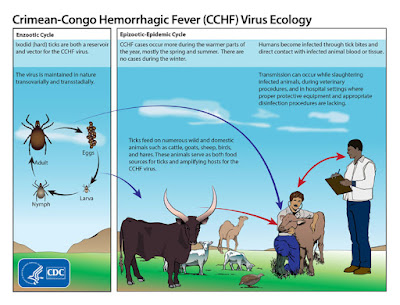 |
| Viral life cycle image via the CDC |
So why are we seeing
CCHF virus labeled as "new"? "New" is the media's historically ignorant term for "emergent", meaning these infectious diseases have been around for a while (some for centuries, even), but environmental and civil factors are influencing spread to new regions. Even the slightest change in seasonal climate or average annual temperature can create a hospitable environment in places that were inhospitable to these disease vectors. We also have a very developed view of the world, where it is hard to see that human actions, such as spillover into forests regions for industrial purposes (extracting natural resources or large-scale plantations for the production of resources), and development purposes (houses, houses, everywhere), can influence the introduction of these diseases to new populations. Not only are the vectors moving into our developed areas, but we are constantly invading and inhabiting natural habitats and contributing to the zoonotic nature of these viruses (and other infectious diseases). After all, we are animals, too.
Forbes, with their obnoxious refusal to let you view articles on their website while using an adblocker plugin,
says that you should be worried about CCHF. The first local transmission of CCHF virus was reported in Spain this year, and the patient died.
A nurse was also exposed as a result of this case, which lead to close monitoring of many people from the medical team and local community. The presence of CCHF virus in Spain has been known since 2011,
when the West African strain of CCHF virus was isolated from ticks in Caceres province. Up until that point, the Balkans were the western-most region known with reported cases of CCHF.
Onset of CCHF is quick, with sudden onset of high fever, severe headache, back and joint pain, stomach pain and vomiting. Patients may appear flushed with red eyes, face and throat, with a patchy red palate. Jaundice and the onset of neurological complications can arise.The hemorrhagic nature of the disease begins with severe bruising and frequent, severe nose bleeds, or uncontrollable bleeding at the site of injection. Outbreaks generally have a case fatality rate of
40 -
50%. Treatment is limited to supportive care, and there are currently no vaccines available to humans or for use in livestock populations.
There are many other hemorrhagic fevers, including Ebola virus (EBOV), Marburg
virus (MBGV), Lassa virus (LASV), Rift Valley fever virus
(RVFV), dengue
virus (DENV), and yellow fever virus (YFV). Differential diagnosis, how we determine which virus is causing the hemorrhagic disease, is very difficult, as many of the symptoms overlap and rapid testing is not always available. In all of these viral hemorrhagic diseases, infection can impact liver cells and liver function. Impairment of liver function can decrease synthesis of protein that initiate clotting. This most likely occurs due to the body's response to severe disease and shock, as more liquid/unclotted blood can disseminate faster to all organs. Infection of liver cells can also cause an increase in clotting proteins, causing small clots to form, blocking blood flow. Hemorrhagic fevers also effect the permeability of blood vessels, causing the severe bruising and bleeding in tissues and orifices, like the nose, gums, or vomiting blood as a result of severe internal bleeding.
If you are following the advice from Forbes, and deciding to worry about CCHF, take action. Check yourself for ticks after spending time outdoors in wooded areas, places with tall grass, or wild animal exposure. Wear long sleeves and pants while spending time outdoors to limit your skin exposure to ticks (you can even treat your clothing with repellent;
learn how here). Lastly, if you find it a tick on yourself, be sure to remove it carefully without pulling the head off or smashing the blood-filled body. If you are worried about disease exposure from said tick, do your doctor a favor and save the tick! It can be sent to a lab and tested, but act quickly as these viruses can be difficult to isolate from old material.